– VISITA
– VALUTAZIONE DELL’UDITO
– TRATTAMENTO DELLE PATOLOGIE:
- Ipoacusie
presbiacusie
improvvise
Acufeni
Otiti
Micosi
Inestetismi
MICROCHIRURGIA E CHIRURGIA ENDOSCOPICA DELL’ORECCHIO
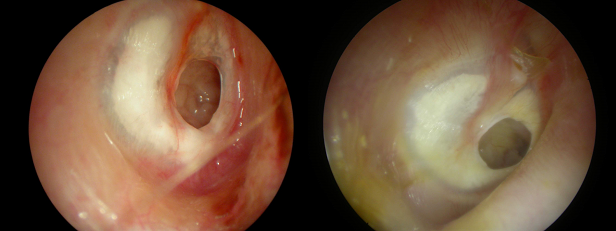
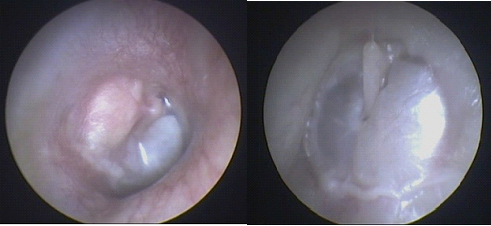
Perforazione timpanica
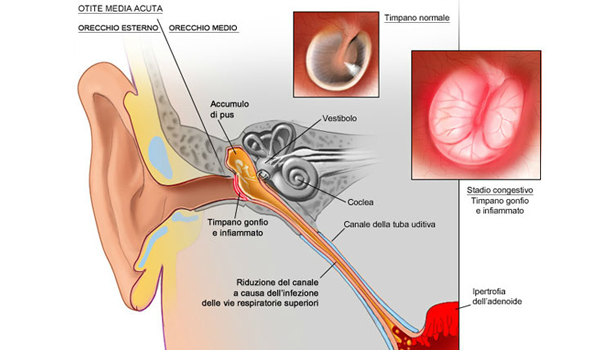
La membrana timpanica è un’importante barriera anatomica protettiva che impedisce a sostanze e microrganismi provenienti dall’orecchio esterno di penetrare nell’orecchio medio ed è un componente fondamentale del sistema timpano-ossiculare che trasmette i suoni all’orecchio interno. La perforazione della membrana timpanica può essere causata da:
• traumi;
• barotraumi (schiaffi, esplosioni, tuffi in acqua, immersioni);
• infezione dell’orecchio medio (otite media acuta o cronica);
• disfunzione della tuba di Eustachio
The perforation of the tympanic membrane usually results in hearing loss transmission more or less accentuated and the risk of recurrent infection in the middle ear.
In many cases the tympanic perforations can repair itself spontaneously, without the need for surgical intervention. In the recent post-traumatic perforations may be useful to run a small outpatient surgery under local anesthesia, which increases the chances of spontaneous perforation closure: it consists in nell'apporre otomicroscopy otoendoscopia or a cellulose patch to hold the tympanic perforation.
In many cases of tympanic perforation it can be indicated the intervention of miringoplastica, executable under local or general anesthesia, in cui la membrana timpanica viene ricostruita in modo parziale o totale mediante l’innesto di materiale autologo contestualmente prelevato, come la fascia del muscolo temporale o il pericondrio della cartilagine del padiglione auricolare.
Otosclerosi
L’otosclerosi è una malattia dell’orecchio caratterizzata da un disturbo distrofico del metabolismo osseo a carico della capsula che riveste l’orecchio interno. La malattia interessa di solito individui adulti, colpendo più frequentemente le donne (in particolare durante il periodo della gravidanza), bilaterale nel 70-80% dei casi. Spesso presenta un carattere ereditario (trasmissione autosomica dominante con espressione variabile), ma esistono anche casi isolati. La patologia è caratterizzata da ipoacusia trasmissiva progressiva, dovuta, nella maggior parte dei casi, al progressivo blocco dell’articolazione stapedo-ovalare (tra la staffa e l’orecchio interno); tale condizione è caratterizzata dalla progressiva formazione di un “callo osseo” alla base della staffa che ne ostacola la corretta vibrazione. Negli stati avanzati si assiste ad una progressiva ipoacusia mista con componente neurosensoriale dovuta all’estensione della patologia alla coclea. Possono essere presenti anche acufeni e vertigini. La diagnosi è principalmente basata sulla storia clinica, l’otoscopia (membrana timpanica normale), l’esame audiometrico ed impedenzometrico (ipoacusia trasmissiva/mista, timpanometria normale, riflessi cocleo-stapediali assenti).
The therapeutic possibilities are nell'otosclerosi:
il follow-up (initial forms, diagnostic doubts, elderly patients and / or systemic contraindications or refusal of the intervention);
the hearing aid fitting, which, however, does not stop the progression of the disease;
in some patients the intake of sodium fluoride appears to be able to slow or even stop the progression of the disease;
surgery stapedotomy. It aims to resolve the transmission component of hearing loss. Under local or general anesthesia, the operation consists in raising the tympanic membrane (tympanotomy exploratory), check the actual bracket block, remove the top of the bracket, then drill a hole in the base of the bracket (platinotomia) and finally positioning a piston prosthesis which is engaged by a side of the anvil and the other positioned in platinotomia. The auditory recovery is in most cases immediate (97% of cases). Nel 2% around there was a failure to improve auditory, while 1% of cases at a hearing deterioration and in very rare cases in total postoperative deafness. Other possible complications are: the temporary or permanent loss of the taste sensitivity of the language related to intraoperative injury of the tympani rope; Transient vertiginous symptoms in the postoperative period; the perforation of the tympanic membrane and the facial nerve deficits are extremely rare.
Otitis media chronic non cholesteatoma
It 'usually characterized by tympanic perforation, inflammation of the middle ear mucosa causing hearing loss, frequent episodes of infection with ear secretion, sometimes tinnitus.
In some cases the intervention of tympanoplasty with or without mastoidectomy can be decisive, allowing you to remove the inflammatory tissue and resolve the causes of the disease. Sometimes the simple reconstruction of the tympanic membrane ensures a good auditory recovery. Sometimes you have to associate un'ossiculoplastica to rebuild a discontinuity of the ossicular chain.

cholesteatoma
A particular form of chronic otitis media is the cholesteatoma, a scaly skin cyst located in the middle ear. Such a condition may be congenital or acquired more frequently for migration of the conduit skin through a membrane perforation or a retraction of the membrane pocket. The distinctive features are the progressive growth of the cholesteatoma with erosion and destruction of the surrounding structures. In addition to the symptoms of otitis media chronic, cholesteatoma may present with symptoms secondary bone erosion: hearing loss and dizziness for erosion of the ossicular chain and / or inner ear; in the most advanced cases of facial nerve paralysis and meningo-cerebral complications. Diagnosis is based on clinical history, l’otomicroscopia, the audiometry. The ear TC is essential in treatment planning which is essentially surgical. There are several surgical techniques, more or less demolitive (closed technique, open, radical) which are selected case by case and adapted to the anatomical characteristics of the individual patient. After surgery you need a close outpatient follow-up to verify the absence of cholesteatoma recurrence. In case of success of the pathology with eredicazione, there exists the possibility of remote perform a second surgical time to reconstruct the eardrum-ossicular apparatus and restore a satisfactory hearing function.
Exostosis of the external auditory canal
New bone formation benign, covered by intact skin and localized at the level of the inner portion of the external auditory meatus. Usually multiple and bilateral, their growth is very slow and seems to be favored by a cold periostitis (Diving and water sports).
E’ indicated a surgical treatment only if the disease becomes symptomatic: Chronic otitis externa, conductive hearing loss for stenosis of the lumen total or subtotal. The surgery, in general or local anesthesia, It is taking out of exostosis through the external auditory canal or, in more difficult cases, with retroauricular approach.
VIDEO
AUDIOLOGIA E VESTIBOLOGIA
edited by Dr. and Dr. B.Mafera. F. small
The Audiology and Vestibular are two otolaryngology branches that deal with the diagnosis and treatment of diseases affecting the ear, the auditory function and vestibular, ie the balance of your body with the surroundings.
Many are the ear disorders that we deal with as, acute and chronic inflammation (scourge), otosclerosi, tinnitus (tinnitus), hearing loss (ipoacusie) of different origin, Meniere's disease, positional vertigo from otoliths (Benign paroxysmal positional vertigo) and other causes and balance disorders (dizziness).
TINNITUS
For Tinnitus is defined as a perceived noise in the absence of external sound sources, It can be perceived in the ear and / or in the head, centrally. In most cases the tinnitus is subjective, that is only perceived by the person who suffers, less frequently it can be perceived externally by the examiner, in the latter case it is somatorumori from the articulation temporo-mandibular, from the vascular system or from muscle.
The etiology of tinnitus can be from otological causes, no otologic but are often idiopathic tinnitus and often multifactorial.
For these reasons, the tinnitus diagnosis should be strict in order to identify the possible etiologies and treatment ,just saying, holistic face to face and treat different causes and contributing factors.
So we face the problem ,"Tinnitus" from a pharmacological point of view, rehabilitation, protesico, behavioral psychology, but also gnathological and osteopathic.
DIZZINESS AND BALANCE DISORDERS
The modern vestibology landscape is one that has recently undergone major transformations through new, modern diagnostic techniques that have allowed us to better identify old diseases and discover new disease entities. Consequently also the therapeutic protocols have been modified to become more and more precise and causal.
Vertigo is a balance disorder, which it manifests itself as the mistaken feeling (illusion) from the environment movement in relation to our body or our body's relation to the environment.
Il termine vertigine indica esclusivamente un sintomo e non la causa della patologia per cui i primo problema che lo specialista si trova ad affrontare è il corretto inquadramento del problema.
La vertigine può essere sia di origine centrale (disturbi del sistema nervoso centrale) che periferica (disturbi dell’orecchio interno) e questo, ovviamente, implica strategie diagnostiche e terapeutiche del tutto diverse.
La sindrome vertiginosa, soprattutto se di origine periferica, è quasi sempre associata a nausea (non di rado culminante in crisi di vomito ), tachicardia e sudorazione profusa; altre volte la sindrome vertiginosa si accompagna a sintomi cocleari (fullness, ipoacusia, tinnitus) e ad emicrania.
LA VERTIGINE PAROSSISTICA POSIZIONALE BENIGNA
It is undoubtedly the most common form of vertigo also known as a root canal lithiasis or otolithic syndrome (canalolitiasi or cupulolitiasi); is determined by a sudden detachment of said small otolith formations inside the rear labyrinth (.
the symptomatology, with abrupt onset and sudden, it is characterized by:
• Violent vertigo roundabouts short (from a few seconds to a few minutes) triggered by the movements of the head and neck and trunk
• Nystagmo (involuntary movement of the eyes) with particular characteristics
• Tendency to recurrence
• Absence of otologic and neurological symptoms
• Presence of symptoms autonomic (nausea, retching, tachycardia) short term.
the diagnosis is made on the basis of a correct anamnesis (typical description of symptoms by the patient) and based on the examination otoneurologico bed_side: maneuvers performed by the specialist with the help of instruments which the Frenzel goggles and / or videonistagmoscopia.
The pharmacological therapy is NOT but consists Specifications maneuvers released able to eliminate symptoms in one or more sessions.